

Summary
This article provides an overview of the specific thinking and actions in psychosomatic osteopathy (PSO) in general and the book “Psychosomatic Osteopathy” by Torsten Liem in particular. Basic assumptions, extended principles, dysfunction models, diagnostic and treatment approaches are explained and differences to conventional osteopathic approaches are explained. Etiological factors, risk factors and mechanisms of action of complaints, healing reactions and soma-physiology-experience-context-dysfunction patterns (SPEKD) are presented in order to develop an understanding of the specific treatment approaches in the context of PSO. The consideration of multiple interdependent and dynamically interwoven influences, holarchic levels of regulation and balance systems in diagnostics and therapy is clinically relevant, as is the identification and differentiation of genetic, epigenetic and metabolic influences. Treatment indications and the treatment structure in the context of PSO are taught. In addition, the particular importance of resources, co-regulation and feedback loops in the treatment setting of PSO is elaborated.
Keywords
Person-context relationship, holarchies, holonic dynamic networks, enactivism, adaptivity, proactivity, principle of energy, dysfunction dynamics, coregulation and feedback loops, somatic dysfunction
Abstract
This article provides an overview of the specific thinking and action in psychosomatic osteopathy in general and the book “Psychosomatic Osteopathy” by Torsten Liem inparticular. Basic assumptions, extended principles, dysfunction models, diagnostic and treatment approaches are explained as well as differences to conventional osteopathic approaches. Etiological factors, risk factors and mechanisms of action of complaints, healing responses and soma-physiology-experience-context dysfunction patterns (SPECD) are presented to develop an understanding of specific treatment approaches in the context of PSO. Thus, consideration of multiple interdependent and dynamically interwoven influences, holarchic levels of regulation, and systems of equilibrium in diagnosis and treatment is clinically relevant, as is identification and differentiation of genetic, epigenetic, and metabolic influences. Treatment indications and the treatment set-up in the context of PSO will be taught. In addition, the special importance of resources, coregulation and feedback loops in the treatment setting of PSO will be elaborated.
Keywords
person-context relationship, holarchies, holonic dynamic networks, enactivism, adaptivity, proactivity, principle of energy, dysfunction dynamics, coregulation and feedback loops, somatic dysfunction
Etiological factors, risk factors and mechanisms of action
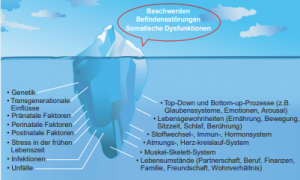
When patients come for an osteopathic consultation, their complaints, disorders and somatic dysfunctions are just the tip of the iceberg. Underneath – often relatively unnoticed – there is a multitude of longer and shorter-lasting, more or less interacting, mutually reinforcing or reducing risk factors, mechanisms of action and allostatic influences (Fig. 1).
Dysfunctional dynamics
The particular organization of our physicality and personality allows us to perceive the world in a certain way and gives us the opportunity to live in the world and take care of our well-being. This dynamic interplay of person and context has developed evolutionarily and genetically, as well as through transgenerational, epigenetic and anthropogenic influences. Our clinical hypothetical working model refers to the fact that both positive or life-enhancing and negative or harmful contextual and environmental influences can occur throughout life (Fig. 2).
Fig. 2: Dysfunctional dynamics. Diagram showing the impact of non-nourishing, negative and harmful contexts
Harmful influences can lead to allostatic reactions, dysfunctional psychophysiological and structural adaptations as well as rigid, outdated conditioning and put a strain on the person’s physiology, reaction and experience patterns, reduce the ability to react adequately and flexibly to current challenges in life and increase the risk of symptoms and illnesses. It is not only the strength and duration of the harmful contextual factors that play a role, but also the time of their occurrence. Early periods of ontogenetic development are particularly susceptible. The earlier in life (including the prenatal period) protective and survival reactions have to be initiated, the more profound inflexibilities and dysfunctional conditioning can result. Polymorphisms also play a role in susceptibility to harmful contextual factors, and the inflexibilities resulting from protective and survival reactions vary depending on the period of life and the intensity and duration of the harmful influences. The analogy of the hardware and software of a computer can be used to illustrate this: The earlier harmful influences occur, the sooner more essential structures can be damaged.- From conception, the hardware can be affected, i.e. genetics.- Fetal programming is illustrated by the functioning of the BIOS (this acts as an intermediary between operating systems and hardware). Here, chronic stress processes of cortisolemia and cortisol resistance affect the unborn child with numerous disease risks later in life [2], [4].- Peri- and postnatal processes could be symbolized by influence on the driver of a computer that controls hardware devices. For example, birth processes affect conditioning in the raphe nuclei in relation to serotonin production [7].- By the age of 4, harmful influences can affect the operating system that manages the interaction of a computer’s hardware and software components. Early childhood stress shows increased disease risks in adulthood as interacting dysregulations in multiple physiological systems impair the ability to respond flexibly to stressful contexts [12]. For example, there are persistent and profound effects on prefrontal, hypothalamic, amygdala and dopaminergic circuits [9].- Disruptive factors in preschool age affect the programs of a computer. Health problems in this period are perpetuated by psychosocial mechanisms [3].In summary, influences in the childhood period are associated with the emergence of certain phenotypes [6], which in turn predispose to certain allostatic response patterns and disease patterns.Consequences of these inflexibilities are multiple prediction errors of inherent feedback systems in relation to internal and external contexts:- inwardly e.g. inwardly, e.g. reactions to alcohol, sports, television, ability-related expectations [5], [8], [11], [13],- outwardly with regard to mentalization processes, e.g. how other people react to the person [10].By encountering new contexts with inappropriate conditioned response patterns and behaviors, experiences are fostered that are non-nourishing, negative and harmful – in the sense of self-fulfilling prophecies – and can lead to further inappropriate dysfunctional protective and survival strategies and inflexibilities. Any prolonged, unresolved dynamic or problem in life can also have an allostatic effect. These can take place on a postural, musculoskeletal, metabolic, immunological (in relation to pathogens and toxins), neuroendocrine, emotional, mental, social, intersubjective (e.g. partnership) or biosocial (work, finances, environmental contexts) level. The consequences can be manifold:- chronic activation and desynchronization of stress axes,- insulin resistance,- increased permeability of barriers,- endotoxemia,- low-grade inflammation,- development of multiple clinical pictures, including chronic pain conditions,- it is seldom possible to identify a single cause. For this reason, anatomical-energetic reductionisms and absolutisms as well as the idea of primary dysfunction or the limitation of therapeutic interactions to a single mechanism of action must be relativized. Rather, it is the sum of all risk factors that increases the probability of disease. This is why we tend to speak of spatially and temporally limited soma-physiology-experience patterns. Therefore, from a clinical point of view, the consideration of an individual dynamic “cocktail” of holarchic top-down and bottom-up interactions – different for each individual – in interaction with part-whole aspects, the person/context structure and with regard to the summation of risk factors and accessible resources over time is essential and indispensable for access to treatment.The mechanisms of action underlying the respective symptoms will initially consolidate functionally, the longer the unresolved dynamics persist, but also structurally or anatomically. Effects and allostatic stress, e.g. low-grade inflammation or dissociation disorders, as a result of chronic stress, stress from early childhood, pregnancy or long-term dysfunctional habits do not necessarily resolve themselves if the reasons for their development are no longer active. In particular, if patterns have become established over many years, it is not enough to rule out and eliminate the original causes or triggers. Instead, mechanisms of action must be identified, differentiated and actively inhibited. At the beginning of the development of osteopathy, these mechanisms of action and their interactions as well as their influence on health were barely known and only rudimentary. For this reason, we currently have significantly more knowledge and therefore osteopathic treatment approaches at our disposal.
Treatment structure
The underlying and associated soma-physiology-experience-context-dysfunction patterns (SPEKD) of the clinical symptoms are treated in a clearly defined setting. The treatment structure in psychosomatic osteopathy is roughly divided into 5 phases: Therapeutic relationship – A clear, stable, transparent therapeutic relationship that supports healing is the basis for all further measures. The focus is on interpersonal interaction and resonance, empathy, solution strategies for obstacles to treatment and attunement to the treatment. Diagnostics – The tissue and physicality reflect the individual’s interconnectedness, perspectives and conditioning. Repressed contents of consciousness or body energies are also expressed in the tissue. By means of palpation, certain parts of the mechanisms underlying the symptoms, complaints and somatic dysfunction patterns can be identified. However, further specialist knowledge and perception tools are required in order to be able to correlate the palpatory findings with the influences mentioned. At the same time, some of these influences cannot be diagnosed by palpation. Further diagnostic skills are required here, such as anamnesis, assessment of behavior, facial expressions and, if necessary, questionnaires, laboratory findings, etc. The diagnostics are geared towards the following aspects:- Recognition of the evolutionary laws and their effect in the current context of the individual,- Assessment of the mechanisms involved,- Identification and differentiation of dysfunctional patterns and the developmental dynamics of the symptoms on the one hand and of resources on the other.The diagnostics are divided into non-palpatory and palpatory examinations. During palpation, for example, interfaces and interactions between body regions, the neurovegetative system, the limbic system, energetic phenomena, psychological experience, the individual’s self-perception and associated contextual factors are explored. Stabilization phase – This includes a variety of skills, e.g. for verbal accompaniment of palpatory approaches, and in particular osteopathic manual procedures for stabilization and co-regulation. Integration/confrontation phase – All the content and skills discussed and presented up to this point are used here. For example, resources are activated, aetiological factors and risk factors are eliminated as best as possible, long-lasting and unresolved dynamics are resolved and ended as far as possible, dysfunctional mechanisms of action – particularly in the case of long-lasting disorders and dysfunctions – are inhibited and PSCD is resolved or worked through. The processing and integration of SPEKD, stress, chronic pain, stress or unprocessed trauma experiences takes place within a clearly defined framework by means of dosed activation and simultaneous co-regulation (aspect of the stability phase) by the therapist. Integration in everyday life – The osteopathic consultation is like a therapeutic uterus. The successful changes achieved there must prove themselves in everyday life. The treatment is also tailored to the extent to which the therapeutic impulses have an effect on everyday life. In the case of chronic symptoms, the healing or, if necessary, the implementation in everyday life happens gradually and is an essential part of the therapeutic effect. These 5 treatment phases are not strictly separated from each other. During treatment, osteopathic approaches are developed and applied in order to activate resource-oriented mechanisms of action or to inhibit dysfunctional mechanisms of action. In addition, patients are given access to attitudes, postures and deep needs that were not previously conscious and accessible by helping them to consciously experience specific reaction patterns in relation to the therapeutic touch. These treatment approaches consist of a measured and fine-tuned real-time interaction of multimodal interactions (palpatory, acoustic, visual, cognitive, emotional, neurovegetative, active and passive movement, interoceptive focus, breathing, etc.). They are used to integrate the aforementioned aspects, e.g. anatomical-physiological interactions, perceptual or sensorimotor states and dynamics. Patients are given co-regulatory support in perceiving, differentiating and integrating these active forces and their relationship to their life context by means of osteopathic palpation. The active participation of the patient is an essential component. This develops and activates the patient’s own co-regulations and sets healing processes in motion. Much depends on the therapist’s sensitivity, “tuning” and ability to resonate in order to allow an appropriate, coherent therapeutic touch and encounter to take place at any point during the treatment. This therapeutic process supports the emergence of emergences with the following consequences:- Relativization and integration of dysfunctional soma-physiological-experiential patterns,- Higher-order organizational levels, increasing complexity and relative autonomy,- Improved adaptivity, e.g. in postural-musculoskeletal disorders. in postural-musculoskeletal, immunological, metabolic, neurovegetative, psychological dynamics and mechanisms of action, with regard to current challenges and contextual changes,- support and activation of the potential for healing and health,- more flexible and proactive postural and behavioral competencies,- minimization of errors in inherent predictive processes,- more adequate and differentiated perception (e.g. of freedom from pain),- increase in proactivity in relation to the context of life.
Co-regulation and feedback loops
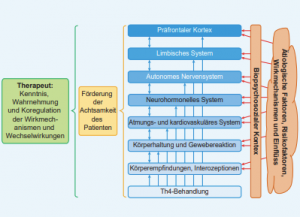
In PSO, therapists act as co-regulators by perceiving neurovegetative, limbic and cognitive reactions of their patients throughout the treatment, e.g. by means of facial expressions, gestures, behavior, posture, breathing, pulse, pupil, speech (in terms of content, emphasis, emphasis, tone, rhythm) [1] (Fig. 3).
Fig. 3: Diagram of the therapist’s role as co-regulator in the stability and integration phase
The resolution of dysfunctional patterns, processing and integration take place in a dynamic state of balance and flow, characterized by effortless attention and an unforced, spontaneous emergent experience of the patient. In the integration phase (as opposed to the stabilization phase), the patient has dosed contact with triggers and dysfunctional aspects of SPEKD, and the treatment approaches take place in a mild neurovegetative arousal of the patient, possibly also in a dynamic balance between negative and positive emotions and between impulse inhibition and activation. At the same time, it is essential to avoid any form of re-traumatization. For this reason, the patient’s proximal learning zone must be identified on the basis of the therapeutic relationship; this refers to the level of integration that is accessible to the patient. In addition, contact with the patient’s subjective experience must be maintained throughout the treatment so that stabilization resources can be individually adapted and applied in doses as co-regulation in the integration or confrontation phase. many other finely tuned aspects of intervention are used during treatment in addition to the touch intervention. In addition, the patient’s proactivity is actively encouraged and inner experience is used as a therapeutic tool and inherent part of the treatment. This includes a variety of interacting multimodal holarchic top-down and bottom-up interventions and reactions to activate a flow state and, as a result, inner working processes that involve multiple mechanisms of action and feedback loops. For example, this process can give rise to evoked, emergent new postures, activity patterns in body regions, changes in muscle tone, breathing, pulse, circulation and other physiologies. By means of mindfulness support, patients can subsequently be helped to perceive associated new bodily sensations, interoceptions, proprioceptions and other somatic markers. They can also identify interactions with beliefs, belief patterns and feelings. Possible changes to these can also arise, and more flexible mechanisms of action can be established so that potentially expanded co-regulations and levels of perception can ultimately be appropriated in the context of life. In the context of PSO, therapists must pay attention to some interactions (Fig. 4), such as the understanding of mechanisms of action and interactions of body systems and organs as well as the dynamic influences of contextual factors and accumulating risk factors in relation to SPEKD. Interactions must be recognized throughout the treatment and co-regulations applied where necessary. In addition, the patient’s awareness of the associated multiple interactions and the skills of co-regulation and self-regulation should be promoted during osteopathic treatment.
Indications for the approaches of psychosomatic osteopathy
The indications correspond to those that also apply to any other osteopathic treatment, supplemented by a few other symptoms, e.g.:- SPEKD- chronic pain conditions,- secondary chronic injuries,- stress-associated and multimorbid clinical pictures,- chronic functional disorders with psychological components, e.g. learning disorders,- past, stressful experiences, memories or significant parts thereof that occur during osteopathic treatment or palpation,- optimization of the individual’s proactivity and adaptivity in relation to their intersubjective and biosocial life context – based on ego experiences, needs, emotions, life goals, self-efficacy, beliefs, dispositions, etc,- increase in awareness and proactivity with regard to habits, lifestyle factors and beliefs in connection with symptoms, – any symptoms and diseases accessible to osteopathy.Depending on osteopathic competence, PSO also includes the following indications:- negative emotions, fears, phobias and dysfunctional emotion regulation,- addictive behaviour,- processing of biographical backgrounds in somatic dysfunctions,- current triggers and habit patterns that restrict everyday life,- allergies,- irrational negative cognitions,- traumatization. SourceAfter Liem T. Psychosomatic osteopathy. Munich: Urban & Fischer bei Elsevier; 2024. literature[1] Bhatara A, Laukka P, Boll-Avetisyan N et al. Second Language Ability and Emotional Prosody Perception. PLoS One 2016; 11 (6): e0156855[2] Cottrell EC, Seckl JR. Prenatal stress, glucocorticoids and the programming of adult disease. Front Behav Neurosci 2009; 3: 19[3] Dalton ED, Hammen CL, Brennan PA, Najman JM. Pathways maintaining physical health problems from childhood to young adulthood: The role of stress and mood. Psychol Health 2016; 31 (11): 1255-1271[4] Drake AJ, Tang JI, Nyirenda MJ. Mechanisms underlying the role of glucocorticoids in the early life programming of adult disease. Clin Sci 2007; 113 (5): 219-232[5] Lee CM, Fairlie AM, Ramirez JJ et al. Self-fulfilling prophecies: Documentation of real-world daily alcohol expectancy effects on the experience of specific positive and negative alcohol-related consequences. Psychol Addict Behav 2020; 34 (2): 327-334[6] Peters A, McEwen BS. Stress habituation, body shape and cardiovascular mortality. Neurosci Biobehav Rev 2015; 56: 139-150[7] Prakash N, Stark CJ, Keisler MN et al. Serotonergic Plasticity in the Dorsal Raphe Nucleus Characterizes Susceptibility and Resilience to Anhedonia. J Neurosci 2020; 40 (3): 569-584[8] Raman VV. A self-fulfilling prophecy: linking belief to behavior. Ann N Y Acad Sci 2011; 1234: 104-107[9] Smith KE, Pollak SD. Early life stress and development: potential mechanisms for adverse outcomes. J Neurodev Disord 2020; 12 (1): 34[10] Snyder M, Swann WB. Hypothesis-testing processes in social interaction. Journal of Personality and Social Psychology 1978; 36: 1202-1212[11] Sternberg E. A self-fulfilling prophecy: linking belief to behavior. Ann NY Acad Sci 2011; 1234: 98-89[12] Taylor SE. Mechanisms linking early life stress to adult health outcomes. Proc Natl Acad Sci USA 2010; 107 (19): 8507-8512[13] Weaver J, Filson Moses J, Snyder M. Self-Fulfilling Prophecies in Ability Settings. J Soc Psychol 2016; 156 (2): 179-189







